While this website might be dedicated to congenital hydrocephalus, I feel that it
is appropriate to add a page for cochlear implants. The cochlea and other structures in
the middle and inner ear are very delicate and do not always do well under the pressure
that is placed on the head and skull before a child can be shunted. As a result
many children with hydrocephalus are born deaf or with significant hearing problems.
Therefore many parents of children with congenital hydrocephalus will have to face
the decision of whether or not to pursue a cochlear implant for their child.
The Basics
As always, it's best to start with a picture and to begin with the basics. First, you
need to understand how the ear works.
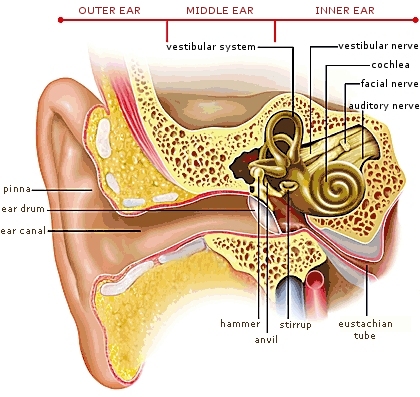
In a normal ear, sound is collected by the pinna (the outer part that you see and
stick earings in) and is directed down the ear canal. The sound hits the ear drum
causing it to vibrate, which in turn causes the small bones of the middle ear -
the hammer, anvil and stirrup - to vibrate. The middle and inner ear are filled with fluid
which allows the vibrations from the small bones to travel down into the snail shaped
cochlea. The walls of the cochlea are covered with small hair cells that translate
the vibrations into electrical signals which are picked up by the auditory nerve and
then interpreted by the brain.
Next we move onto what happens when things are not normal.
One of the most common forms of hearing loss is called sensorineural hearing loss and
it is generally caused by a failure of the hair cells in the cochlea to transmit their
electrical signals to the auditory nerve. This is the type of hearing loss that a
cochlear implant can help with.
So, how does it work?
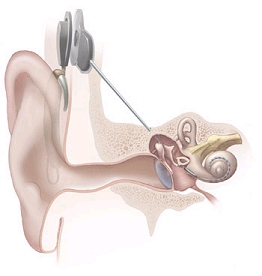
A cochlear implant works by bypassing the outer and middle ear altogether and sends
signals directly to the auditory nerve. The diagram below is from the National Institutes
of Health. In this diagram you can see that the cochlear implant has electrodes which are coiled
up down in the snail shaped cochlea.
A cochlear implant has two parts - an external part with a speech processor and
battery pack that is responsible for receiving sound and an internal part which
is responsible for transmitting those sounds to the auditory nerve. The two
parts communicate with each other through magnets which pass the messages
through the skin via magnetic induction. There is no physical connection between
the internal and external pieces, the skin is completely sealed.
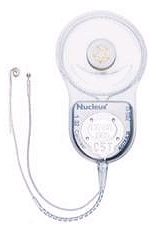
Below is a picture of the external hardware. The piece sticking to the side of
the person's head is called the coil. It is being held in place by a magnet
which sticks to a magnet in the internal piece which is just below it under the skin.
In younger children whose ears are too small to support the
fully "behind the ear" speech processor, a "Babyworn" configuration is used
where there is a
small piece over the ear to place a microphone in the correct position for natural
hearing, but the speech processor and battery are in another piece which can be clipped
to their clothing. Below is little Mariah (thanks to her Mom for letting us use these
pictures, you can read Mariah's story
here) with the Babyworn setup. Mariah has bilateral implants, meaning
that she has implants in both ears, so you can see two processors clipped to her
shirt. From the front it is much harder to see the whole rig. Mariah is wearing the
Nucleus Freedom cochlear implant system from Cochlear Corporation.
The internal piece is surgically implanted behind the ear. If you are not
squeemish you can actually see a video
here
of the surgery done by Dr. Buchman at
UNC-Chapel Hill, who did our son's surgery. Below are the internal pieces of the
cochlear implants by the three major manufacturers:
Cochlear Corporation
Nucleus Freedom
MED-EL
Sonata
Advanced Bionics
Harmony
The internal pieces are very similar between the manufacturers. There is a metal
portion at the top which contains the magnet and the electronics that translate the
signals from the external piece into electrical signals that travel down into the
long probe that comes out from the bottom. The probe is inserted down into the
cochlea and it has electrodes on it that send electrical signals to the
auditory nerve. Each manufacturer has a different number of electrodes and
different shape for the probe, with each
one claiming that their setup is better than the others. In reality they all
seem to work well, and often the choice of which manufacturer to use depends on
the anatomy of the child and the shape of the manufacturer's probes to match that
anatomy.
Concerns for children with hydrocephalus and cochlear implants
Before a child is implanted they go through a fairly long process to determine if they
are a good candidate. One problem that may be encountered is a misshapen cochlea or a
damaged or missing auditory nerve. If your child's hydrocephalus is one of the types that
forms very early in the pregnancy, then it may be that the cochlea and nerve will have
to form under pressure. In order for a cochlear implant to work you need to have an
intact auditory nerve and a cochlea that is at least intact enough to lay the electrodes in.
In our son's case he has no auditory nerve and the cochlea barely got started forming on
his left side. As such he cannot have an implant on that side. On the other side the
cochlea did not fully form, but there was enough to get 20 out of the 22 electrodes
of a Cochlear Nucleus Freedom in and his auditory nerve was fine. An MRI taken
at the beginning of the process will show if the cochlea and auditory nerve are intact.
!!!Remember, if your child has a programmable shunt, it will need to be reprogrammed
immediately after the MRI!!!
Another possible complication for kids with hydrocephalus is if they have a programmable
shunt. Both the internal and external components of a cochlear implant use magnets
to stick the coil to the head and to communicate. Programmable shunts are reprogrammed
using magnets. If the cochlear implant and the programmable shunt are on oppoite sides
of the head, then the internal pieces will not interfere with each other. The external
pieces have to be thought about in greater detail as they can be moved
around and the child could accidentally put it right over the shunt even if the
cochlear implant isn't on the same side. MED-EL makes a magnet for the
external piece that is strong enough to reprogram a programmable shunt and that
magnet should not be used - but all of the models come with choices in strength for the
magnet so it should be possible to avoid the strongest one. The weaker ones do not
seem to be able to reprogram the shunt, or if they do it can only make small changes.
Also, the design of the
Codman Hakim programmable shunt makes it considerably more difficult to reprogram than
the Medtronics programmable shunt. If you have a Medtronics programmable shunt it
may not be possible to use it with a cochlear implant, but I don't have definitive data
on this. A study on programmable shunts and cochlear implants was recently done
at UNC-Chapel Hill. If you need information on this please contact Dr. Craig Buchman's
team in the ENT Department at (919) 966-6484.
Will a cochlear implant restore my child's hearing?
Well, yes and no. Firstly, there is no guarantee that the electrodes will be able to
deliver a good enough signal to the auditory nerve, especially when you are dealing with
a damaged or misshapen cochlea. There is no way to know for sure until you turn it on,
although the surgeon can generally tell you if there is at least a decent enough chance
to warrant the attempt from the MRI.
So lets say you turn it on and walla, the
child reacts to the sound. The next thing to remember is that the normal cochlea has
about 16,000 hair cells in that send signals to the auditory nerve. The implant with
the largest number of electrodes is the Nucleus Freedom by Cochlear and it has 22.
That's less than one percent of the number that a natural cochlea has, so it is not
the same quality of hearing. However new software has done some amazing things with
those 22 (or even the 12 from MED-EL) electrodes and many people are able to understand
speech and even enjoy music. I think of it as watching a streaming video on UTube.
It's not nearly the same quality as on my HD television set, but I can usually figure
out what's going on and get the point that the video is trying to get across.
So after you turn it on it is going to take some fairly intensive speech therapy to
actually achieve the ability to speak and understand what is being said by others.
The most common method of speech therapy for people with cochlear implants is called
AVT, or audio verbal therapy. It emphasizes learning individual sounds first and then
teaches them how to pick out those sounds from words and then how to pick those words
out of sentences. The term "learning to listen" is used quite often in AVT and it
sums up the methodology quite nicely. Whereas hearing people learn to listen naturally,
a cochlear implant recipient has to work much harder at it, mostly because of the limitations
of the implant and also due to the fact that the child is already delayed when they start
because they may not have been hearing properly since birth.
The other thing to keep in mind is that hydrocephalus often brings other learning
delays with it in addition to the ones already caused in the speech area by deafness.
This can have a greater impact on the final ability to acquire speech than the hardware
of the implant itself. In our case we decided that even if our son is not able to
speak in the end, it is still worth it to have him be able to hear us and know that we
are there even when he can't see us. When he is sitting by himself and we are not
in the room we cannot even call out to him and reassure him without actually going
out and standing next to him. During the long car rides to doctor's appointments in
North Carolina (we live in Virginia) he is by himself in the back seat in a rear facing
car seat and he can't see me except a bit in the mirror. I would like for him to be
able to hear me singing to him and talking to him, even if he can't talk back.
What is the process for getting a cochlear implant?
The process starts at birth with the newborn hearing screening. This was not done
for our son because of all of the other issues we had with prematurity and hydrocephalus.
Please make sure that they take the few minutes and do it before your child leaves
the hospital. It is required by law in most states and the sooner you know, the sooner
you can get treatment. Even if they pass the newborn hearing screening you should
probably get a screening done again at six months and one year just to be sure that there
is not a partial hearing loss. Those first months and up to the age of 3 (some say 5)
are really critical to language acquisition and there is such an increased risk of
hearing loss with hydrocephalus that it is something you should pay extra attention to.
If your child fails the newborn screening or a later screening, the next test that will
be done is an otoacoustic emissions test or OAE. An OAE is done while the child is
awake but calm. Ear plugs that are connected to cables are placed in the child's ears.
A computer or small hand held device plays a tone into the ears and "listens" for
an echo that most normal ears produce. This test is very quick and painless and
you should get the result immediately.
If the child fails to produce a response on an OAE then they will be asked to do an
Auditory Brainstem Response or ABR test. It is possible to fail an OAE and still have
hearing, though it is extremely rare. The ABR test is usually done in a hospital
setting because the child must be sedated. Electrodes are placed on the child's head
while sounds are played. If the auditory nerve is receiving sounds it will produce
an electrical impulse which is read by the electrodes. Tones are played at different
volumes and frequencies to test if there is a full or partial hearing loss. An ABR
result is usually considered definitive. It is possible for the re-routing that
occurs in the hydrocephalic brain to produce an unusual response, but most technicians
know that and will try more than one site for the electrodes, though it is something
you might want to mention at the time of the test. Even so, an ABR is generally considered
definitive. If they are hearing anything, it should produce some kind of response, even
if it is an unclean signal because of re-routing.
It is important to note that
there are two different
ABR tests, a "click" ABR and a full tonal ABR. The click ABR just plays single
clicks to test for responses and therefore tests a very small frequency range. The
full tonal ABR tests a much wider range of sounds and will be much more useful. In fact
if they fail the click ABR most cochlear implant centers will require that they go
through a full tonal ABR first thing. As such, I would recommend that you make certain
that the first test is a full tonal one so that you don't have to go through it all
over again later.
One other type of testing that might be done for older child is behavioral testing. In
this type of test the child is put in a sound booth and they are watched for responses
while sounds are played. If they are old enough or capable, they will be trained to
turn their head toward a video screen or a toy that lights up every time they hear a
sound. The training is done with a vibration that comes with each sound at first, and
then when they reliably turn their head the vibration is removed.
You can read more about the testing that is done
here.
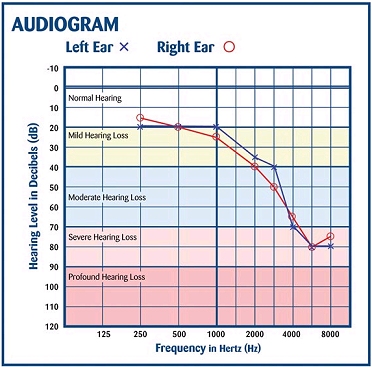
The tests that are done will produce something called an "audiogram". This is a
graph that shows any response at any frequency or decibal (volume) level. If
the child does show some response to sound but not normal hearing, then the audiogram will
be used to set up their hearing aids. If there are no responses the then audiogram
will just be a flat line. Below is a picture of an audiogram:
Even if the child produces no responses on any of the above tests, it is likely that
they will be given a set of hearing aids anyway to use for a trial period during which
they will be tested several times while wearing them. This
may seem frivolous, but it isn't. The placement of a cochlear implant generally
destroys any natural hearing that a person might have. They have to be absolutely
certain that there is not enough residual hearing to be useful. It is also important
to note that even if a child does produce a response on these tests, they may still
be a candidate for a cochlear implant. It is possible to have some hearing, but have
it not be enough to be able to acquire speech. Think of how you hear sounds while
swimming underwater. Your friend can be shouting at the top of their lungs on the
pool deck, but all that you can hear is that they are shouting. You can't make out
the words that they are saying. Or think of hearing someone that is speaking quietly
at the other end of the room. You know that they are saying something, but again you
can't understand the words. For children whose hearing exists but is not enough
for them to understand speech, it may be beneficial for them to receive a cochlear implant.
At some point in this process if it seems likely that a cochlear implant will be needed
then an MRI will be done. The MRI shows the cochlea and the auditory nerve and
will be looked at by a surgeon that can use it to determine if they are in good
enough shape to receive a cochlear implant. REMEMBER! If you have a programmable shunt
it will need to be reprogrammed immediately after the MRI! A CT scan is not detailed
enough to show the tiny little cochlea and auditory nerve, so it has to be an MRI.
Once they have gone through all of the testing and it has been determined that they
are a good candidate, then the surgery will be scheduled. As I mentioned above, if
you aren't squeemish you can view a video of the surgery here:
here. The surgery takes 90 minutes to 4 hours, depending on the
anatomy that has to be worked around. After the surgery huge bandages will be
placed on the child's head. Below is another picture of little Mariah with her
bandages. She had both ears done at the same time, so she has bandages on both ears.
I would have used a picture of my own son, but he managed to get the whole rig off
before I could even get a picture. We had to resort to Mommy running to JoAnn's
fabric and getting some sundress material to stretch over the bandage. And sundress
material doesn't come in boy colors so yes, it's a pink hat that you can just see the
white bandage sticking out from on his right side.
The bandage stays on for 5 to 7 days, or at least you try to keep it on that long.
The hardest part of the whole process starts now, they can't just turn on the device.
Typically you have to wait 4 weeks before turning it on, which is called "hook up".
After the surgery everything needs to heal completely before they start putting
an electrical current through the tissues. Some centers do three weeks and some
go as far as two months, but four weeks seems to be the average. It's very hard
to have the device in, with all the hopes that it brings, and not be able to even
test it out to see if it's going to work.
As of this writing, this is as far as we have gotten in the process. The implant
was put in 4 days ago, but we have not made it to hook up yet. But we have a fairly
good sense of what the process will be from here on out. We have been warned that
the hook up which we are so excited about may not be what we expect. Some children
turn their head when they hear the sound, some cry, some just stop what they are
doing and stare and some may not react at all. They do not start out with the implant
at full volume, they start out with a conservative setting and it is possible that
they might not hear anything at all on the first mapping. It is also possible that
it won't work and that his anatomy won't allow it to produce sound for him.
At fairly frequent intervals for the first few months you will return for new
mappings. Mappings are programs that are loaded into the speech processor to
optimize the output for your specific child. If the child is old enough or capable
the first mapping will be created with their help as they tell you what they can
hear. If they are too young or not capable of communicating what they are experiencing
most of the implants have the ability for a computer to measure the response
without the child's input and that will be used to determine that first mapping.
It may take several mappings to get the settings right for the child to be able to
show reliable responses to sound. The audiograms that were mentioned above will
become very important in determining the changes needed in the mappings.
The final step is lots and lots of speech therapy and lots and lots of work at home.
The speech therapist can teach a parent how to help the child at home. Speech must
be emphasized all day every day in every possible way to maximize the child's exposure
and to help them progress. AVT therapy includes many songs and toys and actions that
are used to teach sounds and the parents can use these at home as well. A great deal
of the outcome is based not so much on the implant itself, but on how much work is
done after the implant is working.
There is a tremendous amount of information out there about cochlear implants
and there are no shortage of web pages covering this subject so I won't bother
to put a list of links here. However I can recommend a video that we bought that
was particularly useful. It's only available on VHS, but it's worth it to dust
off the VCR. It follows two sets of twins, with one born hearing and one born
deaf in each pair, one set are both girls and in the other set both are boys.
In each set, the deaf child is implanted at one year old and they follow their
progress until they are four years old. It is great to see their progress, and it
gives you a true idea of what is involved in acquiring speech with a cochlear implant.
The movie is called Twins and you can purchase it
here.
Legal Disclaimer: While every effort has been made to make certain that the information contained in this website is accurate, it must be remembered that the content is managed by a parent, not by a doctor. Information contained here is for general support purposes only and is no substitute for the care of a physician.