| |
Very early on in our journey I realized that this whole thing
would be an education in new vocabulary. Often I would come home from a
doctor visit with big, long words floating in my head with no definitions
to link up to. Even when the doctor was really good at explaining to us
what the words meant, it was often too much to take in all at once and
I'd be confused by the time we got home. Google was my best friend.
When we got to the hospital after Owen's birth it was even worse. I
remember standing there like a deer in headlights while the nurse asked me
if I wanted to try a PO feeding. I blinked a few times and she repeated the
question. I blinked again. Finally she said, "Would you like to try
feeding him from a bottle instead of through the tube?". I replied, "Why
didn't you just say so?"
This glossary should help you through this sea of new words.
|
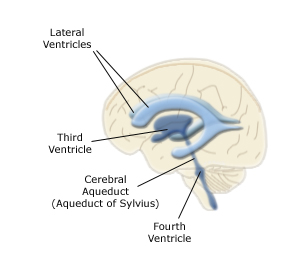
Aqueduct of Sylvius - The very small canal that leads from
the third ventricle down to the fourth ventricle in the brain.
|
|
|
Aqueductal Stenosis - A partial or complete blockage of
the Aqueduct of Sylvius resulting in
the enlargement of the lateral and third ventricles.
|
|
|
Bolus - Administering a substance into the bloodstream in one dose to achieve a desired level
of that substance in the bloodstream. For example, if your child is dehydrated they may administer a
large initial dose (a bolus) of saline fluids to get them back up to normal levels, and then slow it
down to a maintenance dose to keep them hydrated. You will also often hear this term when they
administer antibiotics with a suspected shunt infection if they start with a larger dose to bring
up the level in the bloodstream. Another term for bolus is "loading dose".
|
|
Central Line (also Central Venous Catheter or CVC) - What most people think of
as an IV is more properly called a peripheral line. It is only inserted into the smaller
veins of the arms or legs. These are good for temporary use, but cannot be used long term
or to carry caustic substances such as the antibiotics used for a shunt infection. For
these circumstances a PICC Line or a central line
may be used. A central line is inserted directly through one of the larger veins - subclavian
(under the collar bone), internal jugular (neck) or femoral (upper leg) and completely
bypasses the peripheral veins. There is a greater risk of infection with this type of
line than with a PICC or a peripheral, but they provide much more stable access. The femoral
type carries the greatest risk of infection - due to the proximity to the diaper area I presume,
but the femoral can be placed in a PICU or NICU setup. The subclavian or internal jugular
must be placed in an OR, but they have less of a chance of infection.
There are a few different types
of central lines, named for the type of catheter used. The two most common are the
Broviac and the Hickman. The Broviac is the smaller of the two and is most often used in children.
There is a good description of these two items
here. The other
good thing about a central line is that they can do blood draws through them. This means that
your little one doesn't have to be stuck every time they want a blood sample. Below is a picture of
my son's central line with a Broviac. You can see the line coming out of the chest and ending in a
blue cap that you can screw syringes or IV drug pumps onto:

|
|
|
Chiari Malformation - Click here
for more information.
|
|
|
Communicating Hydrocephalus - In this type of hydrocephalus there is nothing
blocking the flow of CSF from one ventricle to another or from the
ventricles into the spinal areas. Instead, this is a problem
with absorbtion of CSF. Either the ventricles are producing a greater than normal
amount of CSF and it is overwhelming the system, or the parts of the system that
are supposed to be absorbing the CSF are not doing their job.
|
|
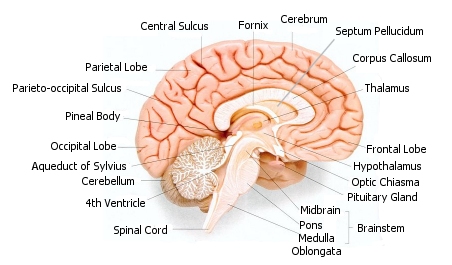
Corpus Callosum - This is a structure of more than 200 million nerve
fibers that provide communication between the left and right hemispheres of
the brain. In some children with hydrocephalus, the corpus callosum may
not be present, or may not fully form. This is called a partial or complete
agenesis of the corpus callosum. The affects of not having a complete
corpus callosum vary widely, but can include cortical blindness, coordination
difficulties or seizures. It may also have very little effect at all.
|
|
Craniosynostosis - A condition where the sutures of the skull fuse together before
brain growth is complete. The skull
of a newborn is not one solid piece, but is instead made up from separate plates that
will fuse later in life.
The sutures are where the edges of the plates come together.
When the shunt is placed, the CSF begins to drain and the plates may overlap. The hope is
that the brain will grow and expand fast enough to be able to push the plates back apart
before they fuse. Sometimes though a suture may fuse before the brain growth can catch up.
After this happens the brain cannot expand evenly as it grows and instead the head
will become misshapen as the brain expands towards the sutures that are still open.
If the condition is not corrected it can eventually cause extra pressure on the brain,
seizures and other issues. For mild cases cranial molds can be used to reshape the head.
More severe cases can require craniofacial surgery to reshape the skull.
|
|
|
Cerebrospinal Fluid (CSF) - Cerebrospinal fluid is a clear liquid that
is produced in the ventricles of the brain. CSF keeps the brain and spinal
cord moist, provides a cushion to prevent damage and acts as a transport
system for waste products and hormones. CSF should flow from the lateral
ventricles to the third ventricle, down to the fourth ventricle via the
Aqueduct of Sylvius and out into the
spinal column where it is absorbed into the bloodstream. Hydrocephalus
occurs either when this flow is blocked and a buildup of fluid occurs,
or when the ventricles produce too much CSF and the normal systems can't
absorb enough to keep the fluid from building up.
|
|
|
CT Scan (Computed Tomography) - A CT scan uses x-rays to produce a
picture of the brain (or other body part). A traditional x-ray used to diagnose
something like a broken bone takes a single picture. A CT scan takes many
pictures called "slices" that are put together to form a detailed picture
of the brain. CT scans can be used to measure the size of the
ventricles to make certain that the shunt is working.
|
|
|
Dandy Walker Malformation - Click here
for more information.
|
|
|
Encephalocele - When an opening in the skull allows
CSF, brain matter and the meninges (the membrane that surrounds the brain)
to protrude from the skull forming a sac. The sac is usually enclosed by skin, however
if there is sufficient pressure it may open. In either case it is repaired after the
baby is born by removing the sac and closing the skin to cover the hole. It then
generally closes on its own as the plates of the skull fuse in their normal fashion,
although some cases may require surgery again later to close the hole.
If no brain matter is present in the sac, it is called a
meningocele.
|
|
External Ventricular Drain (EVD) - The most common use of this device is to provide a
method of draining CSF when a shunt has had to be removed due to infection. It is a
temporary device, used until the infection has been cleared and a new shunt can be placed.
It may also be used when there is a temporary blockage in the flow of CSF due to
something like a head
injury or IVH. A catheter is placed into one of the
ventricles of the brain or the lumbar of the spine and drains to an external drainage bag.
If you would like to see the workings of an EVD in detail from our experience with a shunt
infection click here.
 |
|
 |
|
From the Codman website for the setup of their external ventricular drain
|
|
Thank you to Megan and her family for this picture of an EVD in use
|
|
|
|
Extubate - To remove a breathing tube. See Intubate for more information.
|
|
|
Fixed Pressure Shunt - A shunt whose opening pressure is "fixed". In other words, if
the opening pressure of the shunt needs to be changed, the shunt must be replaced.
See the shunt page for more information.
|
|
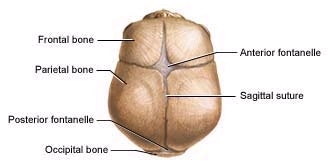
Fontanelle (also Fontanel) - Otherwise known as a baby's "soft spot". The skull
of a newborn is not one solid piece, but is instead made up from separate plates that
will fuse later in life. This design makes it possible for the large head to pass
through the birth canal, and it is also the reason that a baby born with hydrocephalus may
have a large head. The pressure from the buildup of CSF causes the plates to move apart.
There are
a few places in the skull where the plates do not come completely together in a newborn,
leaving open spaces in the bones, and these spaces are called fontanelles. The brain is not
unprotected in these areas, they are covered by an extremely tough membrane.
There are two fontanelles on the top of an infant's skull. The diagram below shows
a top view of
the anterior (toward the face) and posterior (toward the back of the head) fontanelles:
The fontanelles of an infant are very useful in monitoring the health of a shunt. With
a normally functioning shunt the fontanelles should stay soft and
either sink slightly or remain
flat when the infant is upright.
If it sinks down drastically when the child is upright
it can be a sign of overdrainage. If the fontanelle is firm and bulging when the child is
upright then it can be a sign of a shunt failure. Other things can affect the fontanelles
as well. If the infant is fussy the fontanelle may bulge, or if they are dehydrated
it may sink. So check the fontanelle when the child is calm and well hydrated. The anterior
fontanelle is considerably larger than the posterior and remains open for much longer, usually
until about the age of two. As such the anterior fontanelle is usually easier to check.
|
|
Gastric Tube (G-Tube or Gastronomy Tube) - A tube that is placed through an incision
in the abdomen to place food directly into the stomach. A G-tube is generally used when
there is going to be a reasonably long period during which oral feedings will not be
possible, or will not provide enough nutrition to sustain a person in good health.
There are different kinds of G-tubes. The one shown in the picture below is called a
Malecot. This type is often used in preemies and newborns because of the small size of their
stomachs.

|

|
|
Malecot G-tube without clamp
|
Malecot G-tube with clamp
|
|
Thank you to little Cayman and her Mommy for these pictures
|
For older children a button G-tube may be used.
The button type has a balloon that is placed in the stomach which is too large for the real little ones,
but it is much easier to deal with than the long tube of the Malecot.

|

|
|
Button G-tube in place
|
The full button G-tube,
the balloon goes into the stomach.
|
|
|
|
Intracranial Pressure (ICP) - The pressure within the cranium. If CSF is not
draining fast enough, the intracranial pressure will increase. If overdrainage is
occuring the ICP will be lower than normal.
|
|
|
Intracranial Pressure (ICP) Monitoring - A procedure during which the ICP can be
monitored over time. A device is placed inside the head which can measure the pressure
inside the cranium. The test is done while the person is in the hospital and the
device is generally left in place for one to three days. If possible, the pressure is
measured while the person is upright, laying down and sitting to see how the pressure
changes with position. This test can determine if there is over or under drainage,
whether or not a shunt is working properly, or to try
and determine an appropriate setting for a shunt. This test can be done for people who do
not have hydrocephalus who may have a brain injury to see if there is increased ICP.
|
|
Intubate - Technically this means to place a tube into a hollow organ or passageway.
While this could be anywhere in the body, the term is usually used to describe
orotracheal intubation, which is placing a tube down through the mouth to the trachea
(windpipe) or nasotracheal intubation where the tube is placed down through the nose
to the trachea. The tube that is being placed is called a "breathing tube".
It is possible to just have the tube, such as in the case where
a blockage of the airway is suspected, however intubation is generally used in combination
with ventilation. A ventilator is a machine that can "breathe" for a patient by
pumping air in and out of the lungs. While a person is on a ventilator you may hear
the doctors or nurses use the term "breathing over the ventilator". The ventilator is
set to a specific rate for how many breaths per minute it should take. If the patient
is able to initiate breaths on their own so that the rate of breathing is greater than
the rate set on the ventilator, then they are breathing over the rate set on the ventilator,
which is a sign that they may be able to breathe on their own. If you get a nice
nurse they may be willing to show you how to read the monitor on the ventilator so that
you can see which breaths are being initiated by the ventilator and which ones are
being initiated by your child.
Normally they don't just go from having a ventilator doing all or most of the work to
just shutting it off. Instead, they lower the rate of breaths being taken by the ventilator
slowly over time to see if the child will take up the slack and breathe on their own.
When it appears that the child can breathe on their own they will be extubated, which
just means that the breathing tube will be removed. Preemies may need the help of a
ventilator until their lungs mature. Our son needed a ventilator when he aspirated after
throwing up. People are generally intubated during shunt surgery due to the depth
of the anesthetic that is used. For surgery the child is usually extubated before leaving
the operating room, but sometimes the tube is left in if the lungs need some extra time
to breathe completely on their own after the anesthetic.
|
|
|
Meningocele - When an opening in the skull allows
CSF and the meninges (the membrane that surrounds the brain)
to protrude from the skull forming a sac. The sac is usually enclosed by skin, however
if there is sufficient pressure it may open. In either case it is repaired after the
baby is born by removing the sac and closing the skin to cover the hole. It then
generally closes on its own as the plates of the skull fuse in their normal fashion.
If brain matter is present in the sac, it is called an
encephalocele.
|
|
|
MRI - Magnetic Resonance Imaging - There are two types of imaging that are frequently used
with hydrocephalus. CT scans and MRI's. A CT scan uses x-rays to take images
and an MRI uses a tremendously huge magnet to take images. The images taken with an MRI are much
more detailed than those taken with a CT scan and it has the benefit of not using radiation to
produce the images, but there are some down sides to an MRI. It takes a lot longer to
get an MRI - about 30 minutes of imaging time typically - than it does to get a CT scan which takes
about a minute or two of quick images. As such a young child that cannot be told to "hold still" must
be sedated to get an MRI. If the child has a programmable shunt then you have the added complication that
the shunt must be reprogrammed after the MRI since the magnet in the MRI will almost certainly change the
setting on the shunt. There are compelling reasons to use an MRI a however, such
as the fact that a CT scan cannot see detail in soft tissue
the way an MRI can, so at some point most neurosurgeons will want at least a baseline MRI once the tissue
has had a chance to expand. If they are just checking ventricle sizes they will generally use at CT
because it can be done quickly and is just as effective at seeing if the ventricles are increasing in size
when a shunt failure is suspected or for a routine check.
|
|
NG-Tube (Nasogastric) - This is a feeding tube which is inserted through the nose
and goes down to the stomach. This setup is generally used when the need for supplemental nutrition is
expected to be short term. For longer term needs a
G-Tube is usually used. In preemies an NG-Tube is often
used when the baby does not have enough
strength to feed from a bottle or from the breast for a full feeding. Placing the tube
through the nose makes it easier to attempt oral feedings because the tube does not interfere
with the mouth as with an OG-Tube. Below is
a picture of my son with his NG-Tube:

|
|
Neonatal Reservoir (CSF Reservoir, Ventricular Reservoir) - This device is often used
in premature infants where a shunt cannot be placed due to thin skin or a child that is
too unstable for shunt surgery. There are other possible uses for this device as well such as
chemotherapy. Essentially one end of a catheter goes down into the ventricle and
the other end is attached to a silicone "bubble" which is placed just below the skin.
The bubble fills with CSF and can be tapped
repeatedly with a needle to remove CSF to keep the pressure down until a permanent shunt
can be placed.
|
|
|
Non-Communicating Hydrocephalus - The same as obstructive hydrocephalus,
it is caused by a blockage in the flow of CSF.
|
|
|
NPO - This term is related to feeding and the term PO feeding.
Basically when a person is NPO, they are not receiving food or drink via the mouth.
A person that is fed entirely via a tube or IV is said to be NPO. A person is also
NPO during the time when they are fasting before surgery or sedation.
|
|
|
Obstructive Hydrocephalus - Hydrocephalus that is caused by a blockage of the normal
CSF flow through the ventricles or spinal column.
|
|
|
Occipital Frontal Circumference - The head circumference measured at
around its largest area - from above the eyebrows and ears and around the back of the head.
|
|
OG-Tube (Orogastric) - This is a feeding tube which is inserted through the mouth
and goes down to the stomach. This setup is generally used when the need for supplemental nutrition is
expected to be short term. For longer term needs a
G-Tube is usually used. An NG-Tube is usually
prefered because it doesn't interfere with oral feedings, speech or pacifiers. However
it isn't always practical to use an NG-Tube. In my son's case the NG-Tube irritated his
nasal passages to the point where he could no longer tolerate it and it had to be replaced
with an OG-Tube. Below is a picture of my son with his OG-Tube:

|
|
|
Plagiocephaly - Often called "flat head syndrome", this is a flattening along
one side of the skull. In babies with hydrocephalus this can occur because of
positioning in the womb, or when the baby either cannot or does not want to lay
on the side of their head that has the shunt. If they prefer to lay on one side
long enough, a flat spot will occur. Normally this can be corrected by
positioning the baby so that they lay on both sides and the back for equal amounts of time.
If this does not work then an orthotic helmet can be used to reshape the head.
Plagiocephaly should not be confused with craniosynostosis
which is when the sutures become fused, which can also cause the head to become
misshapen.
|
|
|
PO Feeding (Per Oral) - As is mentioned at the top of this page, this is the term that
doctors and nurses use to mean feeding by mouth. This can either mean breastfeeding,
feeding from a bottle or any other food that passes through the mouth.
The term PO feeding is used to specifically indicate that they are not being fed via a tube.
|
|
|
PICC Line (Peripherally Inserted Central Catheter or PIC/C) - This is a type of IV line that is
meant to stay in place for an extended period of time. What most people think of as an IV
is technically called a peripheral IV and is just inserted a short distance
into the small veins of the hands, arms, legs or feet. These lines can only be left in for
a relatively short period of time and cannot handle certain types of antibiotics which are
caustic and will blow out small veins. For these types of situations a PICC line or a
central line is used.
A PICC is inserted through the small peripheral veins of the arm or leg and is then
fed through larger and larger veins until it reaches the large veins around the heart.
A PICC can remain in place for up to a month, although there are some that are left in longer
than that.
|
|
|
Peritoneal Cavity - The space inside the smooth membrane
(peritoneal membrane, or peritoneum)
that lines the abdomen. The organs of the abdomen, such as the stomach and
large intestine, are contained in the peritoneal cavity.
VP and LP Shunts drain into the peritoneal
cavity.
|
|
|
Pleural Space - The tiny area between the two layers of the pleura
(the thin covering that protects and cushions the lungs). Some types of shunts drain into this space.
|
|
|
Polyhydramnios - A greater than normal amount of amniotic fluid
present in the amniotic sac. The volume of the amniotic fluid is evaluated by visually
dividing the mother's abdomen into 4 quadrants. The largest vertical pocket of fluid is
measured in centimeters. The total volume is calculated by multiplying this value by 4.
A higher than normal amount of amniotic fluid can be caused by many things including a
blockage in the GI tract, multiple fetuses, a very large head or certain other defects.
Polyhydramnios is worrisome not only because of the possibility of it indicating that
there is a problem with the fetus, but because preterm labor occurs in
26% of
pregnancies with polyhydramnios.
|
|
|
Shunt Flow Study - A radioactive dye is injected into the reservoir of the shunt.
The progress of the dye as it moves through the ventricular system is then monitored
via a nuclear scintillation camera to
see if it is flowing correctly. This test will determine if there is a blockage in the
normal flow of CSF and is generally used to see if a shunt has failed.
|
|
|
Shunt Series - A series of several x-rays that show the entire shunt system. Shunts
and their catheters have a strip made of a special material that shows up well on x-rays.
A shunt series cannot be used to determine if a shunt has become blocked, but it can
verify the placement of the catheter ends. It can also detect
a broken shunt or if one of the catheters has become detached.
|
|
|
Torticollis - This term is used by physical therapists to describe the condition
where the neck muscles have not developed evenly on both sides, resulting in a head that
is tilted to one side. Toticollis can occur before birth due to positioning in the
womb or because of an abnormally shaped brain or spine or because.
It can also occur after the child is born if the child favors laying on one side
of their head (often the side away from the shunt)
so much that the muscles develop unevenly. Torticollis is generally corrected through
excerises and is one of the reasons that physical therapy is stressed so heavily
right from birth.
|
|
Vancomycin - An antiobiotic that you may encounter if your child has a shunt infection.
This is a fairly nasty one and is rather caustic to the veins. As such it should not be administered
for more than a very few doses through a peripheral IV. If Vancomycin is ordered then you should make
certain that a PICC line or a central line is also
ordered because it's not really a question of "if" the Vancomycin will blow out the peripheral, it's
more of a "when". Nurses and doctors will often refer to Vancomycin as just plain "Vanc". One of the more
nifty side effects of Vancomycin is called "Red Man Syndrome". Vanc will often cause the child to turn
a rather bright shade of red from head to toe (I really wish I had thought to take a picture
when Owen did this, it was quite impressive). I am also told that it produces a rather unpleasant itching
sensation. To combat this, the nurse may give your child a dose of Benedryl just before the Vancomycin
which seems to work well, and it gives you an extra hour of nap time.
Vancomycin is a drug that will
generally be used only if a culture specifically shows a bacteria that requires it. The reason is that
this drug is kept in reserve to use against the most drug resistant strains of bacterias (such as MRSA).
The more a drug is used, the more likely that bacteria will become resistant to it. Vancomycin must also
be kept at a fairly high level in the bloodstream to be effectively absorbed by the CSF. Therefore it
is likely that blood tests will be ordered every few hours for the first few days of use to make
certain that the levels are staying up until they learn how your specific child absorbs it. They
are also checking to make certain that the levels don't get too high, which can cause kidney damage.
|
|
|
Ventilator - A machine that can help a person breathe. See Intubate
for more information.
|
|
|
Ventricular Tap - There are some circumstances under which it may not be possible to
place a shunt or a reservoir, but where it is important that CSF pressure be reduced immediately.
A common case would be a very premature infant that is too unstable for surgery. During
a ventricular tap a needle is inserted directly into a ventricle to remove CSF. This procedure
can be repeated as needed to relieve pressure until a more permanent solution can be done.
|
|
|
Ventriculomegaly - Ventriculomegaly literally means
"enlarged ventricles" and it refers specifically to enlarged lateral ventricles. It is possible to have
enlarged ventricles without any symptoms. When symptoms begin to appear it is then called
hydrocephalus. Many people will use the terms interchangeably, but there is technically a difference.
|

















