Hydrocephalus occurs when there is an excess buildup of cerebrospinal
fluid (CSF) in the ventricles of the brain. The job of the shunt is to
provide a path for that excess fluid to drain.
The shunt itself is
a valve that is connected to two catheters. The parts of a shunt system
are:
Proximal Catheter - this catheter is placed
in the ventricle that is enlarged and is called the proximal catheter.
Occasionally the proximal cathether can be placed in the lumbar of the spine
which is often done when the ventricles are too small to accomodate a catheter.
Shunt Valve- This is the actual hardware that
maintains a constant intracranial pressure (ICP) by allowing CSF to drain
in a controlled fashion. The proximal catheter connects to one end of
the shunt valve and the distal catheter connects to the other end.
Distal Catheter - The distal catheter starts at the shunt
valve and can terminate in several different locations
depending on the circumstances.
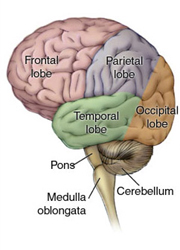
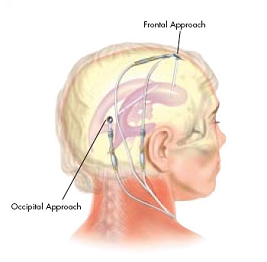
The proximal catheter can be placed in several locations and the approaches are
named for the lobe of the brain that the catheter is inserted through.
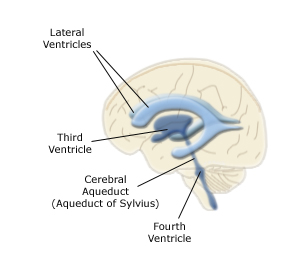
The diagrams below show the lobes of the brain and placement of
the proximal catheter and shunt valve. The diagram on the right, which is
brought to you courtesy of the Johnson & Johnson Codman website,
only shows occipital and frontal, but parietal is also a possibility.
The medical illustration is provided courtesy of Alzheimer's Disease Research,
a program of BrightFocus Foundation.
To make this a little more real, below are two pictures of actual
infants:
A frontal shunt placement (thanks Eli!)
A parietal shunt placement
Where the proximal catheter and shunt valve are placed is dependent upon
which ventricles are enlarged, the structure of the skull and the
neurosurgeon's preference. Once the hair grows out the shunt is
much less noticeable.
The next thing to look at is the shunt valve itself. Most people don't
bother with the valve part of the title, if someone says shunt this is
the part that they are talking about. Shunts are designed to maintain a
specific intracranial pressure. This is also refered to as the
"opening pressure" of the shunt because it is the pressure at which
the valve will open to allow CSF to flow. The opening pressure
is generally expressed in mm H20 (millimeters of water).
There are two basic types of
shunts:
Fixed Pressure - The opening pressure of these shunts
cannot be changed. If a change in pressure is required due to
over or underdrainage, surgery must be done to remove and replace the shunt
with a new one. Typically the fixed pressure shunts come in three
different settings: high, medium and low.
Programmable - The opening pressure of these shunts
can be changed via an external magnet so that surgery is not necessary
for a pressure change. There are two manufacturers of programmable
shunts, Codman (a Johnson & Johnson Company) which has 18 different
pressure settings and Medtronics which has 5. The one down-side
of a programmable shunt is that large magnetic fields can change the
pressure setting. As a result, if an MRI is needed the shunt will need
to be reprogrammed immediately following the MRI. This does not
mean that an MRI can't be done, it just means that you need to set up
having the shunt reprogrammed ahead of time. Reprogramming is very
simple, they just lay a device over the shunt and push a button, then
use an x-ray to verify the setting. I have had several people ask about
accidental reprogramming. This is incredibly rare and you can read more
about this in a 7 year study about the overall performance of the Codman
Hakim Programmable valve
here.
I do not have similar information on the Medtronics valve, if anyone has any such
links please send them to me.
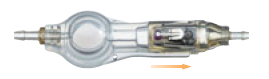
Below are pictures of two shunts made by Codman. The picture on the
left is a fixed pressure shunt and the picture on the right is a programmable,
and also happens to be the exact shunt that our son Owen has:
Most shunts have a small resevoir so that the shunt can be "tapped".
This is a term you will hear often and it is when the neurosurgeon
places a small needle into the resevoir to take a sample of CSF.
A shunt tap can provide information on intracranial pressure and the
sample of CSF removed can be tested for infection. They can also
inject a radioactive dye into the shunt system so that the flow of CSF
can be tracked to determine if the system is working correctly.
You will often be asked the question "What type of shunt do you (or does your
child) have?". You could answer with programmable or fixed pressure, but
most likely what the person is asking is, "Where does the proximal catheter
start and where does the distal catheter end?" Most
proximal catheters are placed in one of the ventricles of the brain and
those shunt system names start with "ventriculo". If the proximal
catheter starts in the lumbar of the spine, the shunt system name will
start with "lumbo".
Where the distal catheter terminates is how you get the second half of the
name for the shunt system. The most common place is in the
peritoneal cavity, which is the space surrounding the stomach. If the
distal catheter ends here, then the shunt system name ends with "peritoneal".
In infants
and young children extra catheter tubing is coiled up in the peritoneal
cavity so that the catheter need not be replaced as the person grows.
If for some reason the peritoneal cavity cannot be used, such as
when there are problems with the stomach, then the next most
common place is the right atrium of the heart. The name of these
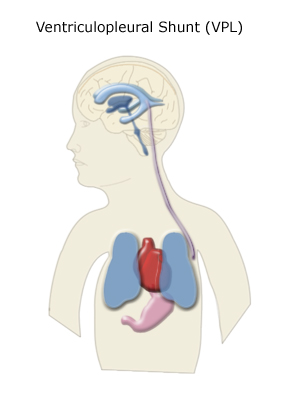
shunt systems ends in "atrial". The final place where
the distal catheter can be terminated is into the pleural space
that surrounds the lungs and those shunt systems end in "pleural".
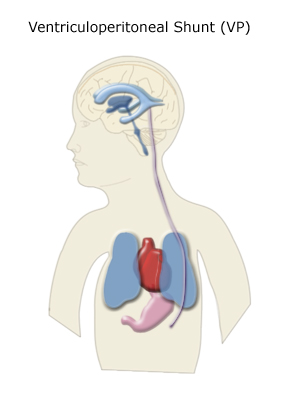
So the most common shunt system that starts in a ventricle and ends in the
peritoneal cavity is called a ventriculoperitoneal shunt or VP shunt.
If the same system terminates in the atrium of the heart it is a
ventriculoatrial or VA shunt. If it terminates in the pleural space then
it is a ventriculopleural or VPL shunt. If the system starts in the lumbar
space and ends in the peritoneal cavity then you get a
lumboperitoneal or LP shunt, and so on.
Anti-Siphon Devices
In the diagrams above you can see that the proximal end of the catheter is generally
placed much higher in the body than the distal end. When a person is upright this
setup allows gravity to pull the CSF down through the valve system, which is known
as siphoning and is a major cause of overdrainage.
To counter this an anti-siphoning
device may be used. This device may either be built into the shunt valve, as is the
case with our son's Codman programmable valve, or it may be a separate device placed in
the shunt system. These devices are designed to even out the flow as the person changes
position.
Shunt Failure
Shunt failures are something
that one has to be constantly on the lookout for. The rate of shunt failures in children
under the age of one is very high. Even though it lessens over time, it never really
goes away. Everyone who has a
shunt or who cares for someone with a shunt should know the signs and
symptoms of a shunt failure. When a shunt fails it no longer allows the
appropriate amount of CSF to drain and therefore the CSF will start to
build up again putting pressure on the brain.
The classic symptoms of a shunt failure in an infant include:
Sleepiness or lethargy
Increase in head circumference
Fontanelle (aka soft spot) is bulging and firm when infant is
sitting upright and calm
Irritability
Vomiting
Swelling along the shunt tract
Downward deviation of the eyes
Prominent scalp veins
Loss of previous abilities
Seizures
Headache
Loss of balance
For older children and adults you can also look for a change in vision, which
is harder to spot in the little ones.
For infants who still have an open fontanelle (soft spot), pay close attention to
how it behaves when everything is fine so that you will know that it
is behaving differently when something goes wrong. It should sink down a bit and be
soft when they are upright, and bulge slightly and be firm when they are lying down.
Each child will have a different norm, so it's important to know what that norm is
so that you can recognize when it changes. If the fontanelle stays firm and bulging even
when they are upright then there may be a problem. If it sinks down drastically and
continues to sink down when they are upright then either they are dehydrated or they
are overdraining (see below). Try giving them some extra fluids to see if the soft
spot returns to normal.
During the years before the soft spot closes you should also
measure their head
circumference regularly to look for sudden increases. It will vary by a few millimeters throughout
the day and that is normal. It can also be difficult in really young infants because their
head shape will often change throughout the day or across a week. So try to measure in the same
spots every day, and look for dramatic changes such as more than a centimeter in one or two
days.
I have had parents describe shunt failures that follow the classic symptoms and
were easy to spot. The one shunt failure we have lived through started out
with a buildup of the CSF along the shunt track for a month or so as the
catheter slowly clogged up before it finally failed completely. At this point we very
quickly went to having a good number of the classic symptoms including
increase of head circumference, bulging fontanelle, vomiting and
sleepiness. I have had other parents say that their child showed none
of the classic signs and they were just able to tell because their child
started acting differently.
The most important thing to remember is that if you think something might be
wrong you should have a neurosurgeon check it out. It's better to go
in and have them say, "Nope, nothing wrong" than to risk possible brain
damage due to a shunt malfunction.
Shunt Infection
I placed infections in a separate section because it is quite possible to
have a shunt that is working properly that also gets infected. Most
shunt infections occur within three months of the shunt placement, but
it can happen at any time. A fever with no other obvious cause, especially
soon after a shunt placement should be checked out. Redness or swelling
along the
shunt tract is also something to watch out for and should be
reported immediately. Remember that shunts are
placed in the brain and if they get infected, the brain can get infected.
So take any indication of a shunt infection seriously and call your
neurosurgeon promptly. If there are active symptoms of a shunt infection
you should probably call your neurosurgeon while driving to the
emergency room as these infections can be deadly.
If an infection is suspected the shunt can be "tapped", meaning that
a small amount of CSF can be removed by placing a needle into the
resevoir of the shunt. The CSF can then be tested for infection.
If a shunt becomes infected, the general procedure is
to remove the existing shunt system and place an external drain while
antibiotics are given for about a week to clear up the infection. Once
the infection is gone a new shunt system is placed.
Now having said all of this about shunt infections, you do sometimes have
to do a reality check. People get sick without it being a shunt
problem and in the wintertime children can get sick often.
You really don't want to be freaking out about the shunt every time
they get a basic childhood illness. For example, I brought Owen into
the pediatrician with a temperature of 104 with no other obvious symptoms.
It wasn't his normal pediatrician, it was just the doctor on call. She
immediately said that we should take him to the local neurosurgeon to
get the shunt tapped and not even wait for a trip down to Duke.
I explained that while the odds were not zero of
it being a shunt infection, the fact that it had been a year since his
shunt was placed meant that the odds of it being something else were far
greater. She settled for just calling Dr. Grant, Owen's neurosurgeon down
at Duke, who basically told her the same thing that I did.
What the pediatrician did not take into account is the fact that tapping
a shunt is not without risk. If the child has an active infection or virus
and you put a needle through the skin to the shunt, you risk introducing
that infection or virus into the shunt system - thus causing the exact thing
that you were worried about. You could walk into the shunt tap with a case of
roseola, which is what Owen turned out to have, and walk out with a shunt
infection. So if there is no redness or swelling along the shunt tract and
it has been a while since the shunt was placed, it is probably best to
rule out other things before tapping the shunt.
The general procedure seems to have been that if Owen
had worsened he would have been admitted to the hospital for observation, but
probably still would have waited for the tap until the lab tests for all
other normal illness possibilities had come back negative. If the shunt has
recently been placed then you should suspect
a shunt infection much more quickly.
We actually experienced a shunt infection and if you would like to read about
the details of what happens with one you can click here.
Over or under drainage
It is possible for the shunt valve to be working properly, but to have the
pressure setting not be appropriate. There must be a balance between the
amount of CSF that is being produced and the amount that is being drained.
Drain too much and the brain tissue loses its support and can collapse
inward, drain too little and the pressure builds up. The pressure setting
required to maintain this balance can change over time.
If the CSF is being drained more quickly that it can be replaced,
overdrainage occurs. In infants you can look for a fontanelle that sinks
considerably when the child is sitting or standing. It will normally sink down
a little bit, but if it sinks radically or sinks and continues to sink
there may be an overdrainage problem. In any age you can look for
irritability when sitting or standing that goes away when they lay down.
Underdrainage looks pretty much like a shunt failure in the sense that
the symptoms are the same. The only difference will be that when the
shunt is tapped or replaced it will be found to be functioning properly.
If the shunt is programmable different pressure settings can be tried
to see if that alleviates the symptoms. If the shunt is a fixed pressure
type it will need to be replaced to change the setting. In this case
the neurosurgeon may try Intracranial Pressure (ICP) monitoring first
to determine the actual pressure inside the brain before putting in a new
shunt.
A Note for New Parents
It is important that you know what type of shunt system your child has,
the make and model of the shunt and
whether or not it is programmable. If it is programmable
you should receive a card at the hospital that tells you
what the current pressure setting is and you should make sure it gets
updated each time the pressure setting is changed. If you
are traveling and have a problem, or have to go into the emergency room,
it is much better to know this than to have to wait for someone to look it up
or to call for records. It is also a good idea to have your own copies of the
last few CT scans or MRI's. This way you can bring them with you when you
travel. Without a past scan to compare to, there is no way to know if
the ventricles have enlarged if you suspect a shunt failure. It could
take some time to get these records if you are at a different hospital
than your normal one and a lot of precious time could be wasted.
The last thing to make certain of before you leave the hospital is who
you should contact in case of an emergency with the shunt. Do you just
call the neurosurgeon's office, or is there a special after hours number
for an on call service? If your preferred neurosurgeon is several hours away from
home, is there a local neurosurgeon that can act as a backup for small
things like checking an incision? Having all of this put together ahead of
time will bring peace of mind knowing that you are prepared.
Legal Disclaimer: While every effort has been made to make certain that the information contained in this website is accurate, it must be remembered that the content is managed by a parent, not by a doctor. Information contained here is for general support purposes only and is no substitute for the care of a physician.