There are a lot of very nice websites out there that cover seizures and Epilepsy in detail and I am not going to try and outdo
them. For more information than you could ever imagine on Epilepsy as well as a good community of people I recommend
Epilepsy.com. I do feel that since so very many kiddos with hydrocephalus also
have seizures that I should at least go over the basics here, and to point out the areas where hydrocephalus can make seizures
a bit more complicated. Remember, not all kids with hydrocephalus will have seizures so
there isn't necessarily a need to panic if your child isn't having them or your child is
as yet unborn - just read the "How to Spot a Seizure" section and take the classes in the "What
Should I Be Doing" section at the bottom to be prepared and don't worry about the rest
until/unless your child starts having seizures.
How To Spot a Seizure
The first question everyone asks is - "How do I know if my child is having a seizure?" And this
turns out to be harder to answer than
you might think. On TV the seizures are always the same - a person falls to the ground and starts
flailing wildly, and occassionally they
even add a bit of frothing at the mouth for extra effect. These scenes depict what used to be known
as a Grand Mal seizure, and
is now known as a tonic-clonic seizure. That is what they look like in an adult - minus the
frothing at the mouth. As it turns out
this is only one type of seizure and there are in fact many, many different types of seizures.
As our neurologist once described to me:
"Anything that the brain could normally make your body do at your request it can also make you
do without your permission and that
is a seizure." You could search every seizure type shown on Epilepsy.com and you won't find
anything that describes the seizures that my son has. I knew a kid in elementary school who
would get stuck in a loop doing whatever it was he had been doing when the seizure hit, so
he would just pick up his pencil, put it down, pick it up and put it down
and repeat that motion until the seizure cleared.
So there is no way I can say: "Look for this and if you see it that is a seizure." But there
are some general guidelines.
Rythmic movements:
The convulsions that come with some types of seizures
can be very difficult to spot in infants. The big Hollywood motions that you see
in older children and adults don't usually happen in infants simply because they have
not yet built up enough muscles to achieve them. In infants and very young children
you tend to see twitching instead and it may be quite subtle.
But all of us twitch at some time or another, especially
when we are falling asleep and just a little twitch doesn't usually mean anything.
If that twitch continues in a rhythmic fashion however then there may be a seizure. When you
are shivering from the cold it is kind of a random motion designed to warm you up, but
seizure tremors or convulsions tend to have a very distinct rhythmn to them.
You might also see that the tremor starts in one small area of the body such as one hand
or foot or an eye and then other areas of the body join in.
Change of conciousness:
This one sounds vague and that's because it is.
We all have moments when we daydream and seem a bit "out of it" and that doesn't
mean we are having a seizure. How do we know the difference? The biggest thing to
watch for is
whether or not the change can be interrupted. It may be that the change is to
absolute unresponsiveness - not to be confused with unconciousness, the person may
seem fully awake and still be sitting upright. In the case of absence seizures
the person simply stops responding to all stimuli for a brief period of time.
During this time they may simply stare, or they may make repetitive motions but they
will not respond to any attempts to get their attention. It may also be that the
change is more subtle. During partial seizures the person is often awake and aware of
what is happening - my Owen often begins his episodes as a partial seizure and he will
still accept a toy from you if you try to hand it to him and yet you can tell that he's just
not all there. He has difficulty making eye contact and his movements seem vague during
these times. The important point here again is that tapping him or saying his name does
not change his state, he will remain vague until the seizure resolves.
Sudden change in muscle control: And by this I mean VERY sudden. There are a few
types of seizures that fall into this category. During an Atonic seizure (formerly
known as "drop seizures") the person's muscle tone suddenly disappears. It may just
be an eye that droops or the head may nod, but if it affects the legs and the person
is standing then they will suddenly drop to the floor. If they are sitting they
may suddenly slump over. The opposite behaviour would be Myoclonic seizures which
are quick jerks that may occur singly or in clusters. Unlike convulsions which take up
a rhythmn and tend to last for at least a minute (and can last for 20 minutes or more)
myoclonic jerks are a quick movement. Everyone has these to some extent - hiccups and
the little jerks you make when you are falling asleep are examples - the problem
is when these involuntary movements start interfering with your voluntary ones. And
finally I have to mention Infantile Spasms in this category. They are also sudden
movements such as a bobbing of the head, bowing from the waist (while sitting),
drawing up of the knees, extending the neck or arms or legs, or crossing of the arms.
These movements often come in clusters, though not always. These are a particularly
devastating form of seizures that usually start between 4 and 6 months old, but can start
as late as 2 years old. The problem is that Infantile Spasms quite often cause significant
brain damage over time and it is not unusual for a child to regress in their abilities.
Children with any of these seizures that cause sudden changes in muscle control will often
wear helmets to keep them safe from head injury.
Even having said all of this, it can still be hard to know if something is a seizure. My son's
seizures in the beginning met none of those criteria. He would usually throw up and then go to sleep.
We didn't think anything of it. Once when he was about 19 months old we found him in his crib
with a lot of vomit and he wasn't breathing. We assumed he had aspirated the vomit. Then
when he was almost three we heard him throw up and saw him slow his breathing way down - without
any outward sign that he had aspirated and we finally realized that it was an autonomic seizure.
And then we realized that all those times that he had thrown up and then went to sleep in the
previous year and a half were probably him having a seizure and then going postictal (deep
unconciousness that you can't wake them up from). He didn't start having tremors with his
seizures until he was three, and didn't start having Hollywood convulsions until he was four.
How Can I Tell For Sure?
Some types are fairly obvious to see - if you get a plain old tonic-clonic (grand mal)
seizure it can be pretty straightforward to guess what is going on. For just about anything
else then you need an EEG (Electroencephalogram) to be absolutely certain. When they
do this they use some goo - looks and feels like Vasoline - to stick a whole bunch of
electrodes to your child's head:
During a short term EEG they usually like the child to be asleep while they put the electrodes
on and may give them a mild sedative to achieve this. They monitor for a little while as the
child sleeps and then they wake them up to watch the brain activity as it changes its
state of conciousness. The threshold between awake and asleep is a very common time
for seizures to occur. They will then monitor them for a little bit while they are awake. These
tests are done in one day on an outpatient basis. If you child has infrequent seizures or
if meds have not worked and they need to try and get some in depth information your
neurologist may have you admitted to the hospital for a long term study that can last for a few
days or even a few weeks. The neurologist can read the EEG - which looks like a bunch of
wiggles on a page - and see if the patterns show abnormal activity.
Treatment
There are a few basic types of treatments for seizures:
MEDICATION
Meds are generally the first thing that neurologists try
in their attempts to combat seizures.
There are hundreds of different seizure meds and I can't possibly list them all here,
so what I will try to do is to discuss them in more general terms.
As we all know the brain works by sending electrical messages that control the body.
Those electrical impulses are created by various chemicals that the body produces.
Seizure medications attempt to change those chemicals so that they alter the
way they produce messages. Some attempt to suppress activity and others attempt
to change the nature of that activity.
There are three different classes of medication -
emergency (aka rescue) meds, short term preventative meds and long term
preventative meds. Now I'll admit that those are my own homemade terms, but
I think it is helpful to understand these concepts because you use these
different classes for different reasons.
Emergency or Rescue Meds:
Used after a seizure starts and only if a seizure doesn't
stop on its own. The most common form of rescue med is
Diastat which is Valium that is given rectally. Diastat
is usually not given to children under the age of 6 months for
two reasons: 1) Most infants can't get a long lasting seizure
going because they don't have enough synaptic complexity in
their brain yet and 2) How to put this delicately? Their
little bottoms aren't quite big enough to handle the
applicator yet. For the rare cases where a rescue med
is needed for a child under 6 months a Versed nasal spray
can be used. I have a personal view that every home that
has a hydro kid older than 6 months should have Diastat in
it. The risk of these kids having at least one major seizure
in their life is quite high and seizures generally show
up in a rather unannounced fashion. Diastat has a long shelf
life and it can just sit on your shelf unthought of
until/unless you need it. I don't know that many docs
would agree with me, this is just my own humble opinion.
Long Term Preventative Meds: No I haven't forgotten
the short term ones, it's just easier to explain them in this
order. The long term meds are probably the first ones that
you think of when someone mentions seizure medication. This is
the stuff that you take every day in hopes of preventing a
seizure from ever happening again. In infants the first
choice is often phenobarbital which has the longest safety
record in infants and has a high success rate. The downside
is that it is also very sedating and therefore isn't often
used in older children. In older kids the first med choice
is usually Keppra because it has a high success rate and has
relatively few side effects for most people and has none of
the nasty physical side effects like liver damage, rashes,
vision damage and other lovely things that some other meds
bring with them. These are just popular choices and may or
may not apply to your specific case - there are hundreds of meds
for neurologists to choose from. Finally it should be noted here that
long term seizure meds are almost never
discontinued in a sudden fashion. In general they must be weaned slowly
over time. The meds change the way that a brain works and a sudden change
can bring on seizures all by itself. So seizure meds are brought on
slowly and weaned off slowly.
Short Term Preventative Meds: These meds fall in between
rescue meds and long term meds. You don't take them every day, but they
are not as hard hitting as the rescue meds. You also don't need to ramp them
up or wean them. I can think of two different
cases where these are used. The first would be if your child is the sort
that "telegraphs" that they are going to have a seizure. Some kids
will start acting oddly for a while before their seizure hits so that you
have some advance warning. In this case you might be able to give them
a single dose of something like Clonazapam to head off the big seizure. It's
a tab that dissolves in their mouth and while it is a bit sedating, it won't
knock them out like the Diastat does. The other case is for children who
have illness as one of their triggers. Triggers are events that bring on
seizures - they can be anything from flashing lights, certain sounds to being tired.
Illness is another common trigger either due to febrile seizures (seizures that
occur while you are running a fever) or because the immune response sets
off a seizure. For these kids it is sometimes necessary to add doses of
Ativan or Clonazapam (or a few others) during the illness while they are at their
highest risk.
All seizure meds carry
the possibility of some type of side effects. These medications work
by altering the way
the brain passes its messages about and you can't imagine that you can
do that sort of thing
without there being the potential for unwanted issues. Some kids will
have minimal to no
side effects even at high doses, others will be incredibly sensitive
and react to even tiny
amounts. The same drug that stabilizes one child will cause the next
one to have behavior
problems. There is no way to predict the way a particular drug will
affect a particular child so
prescribing seizure meds is more of an art form than a science.
All forms of seizure control are a balancing act between side
effects and benefits. As such the neurologist will most likely
start your child at a relatively low dose of any particular med and
then slowly increase the amount if seizures continue. They will
continue to increase the dose until 1) the seizures stop, 2) it
becomes obvious that the med isn't helping at all or 3) the side
effects become too severe. Once a new med is started they may or
may not discontinue the old one. Many times a med will work differently
when used in concert with another one and they will try combinations.
Something else that you need to be aware of is product labeling. No, I don't mean the
actual label on the bottle, but the way medicines are listed with the FDA. Getting FDA
approval for a medication is a long process that consumes a great deal of money. Almost
every product out there is approved for adult use first - this is because it is much easier
to get approval to test on adults and the testing costs a lot less money. Once they have
approval for adults they almost never move immediately to get approval for children - it simply
costs too much. Doctors however can prescribe medicine for off-label usage if the situation
makes it seem necessary, like when nothing else has worked or if they know that it
has been used "off-label" safely with many other children. So the drug companies usually wait
for the doctors to use the
products for a number of years in children so that they have data to go to the FDA with, or
they just never bother because they are getting all the income already without the approval.
As such there are many seizure meds out on the market that are labeled "Not for use under the
age of 18", or 15 or whatever they were approved for, but have been used for years on much younger
children. These include some of the best seizure meds out there so don't be surprised if you
Google one of your meds and find that someone says it shouldn't be used in young children.
If you have concerns ask your doctor instead and discuss with him how long a drug has been
used in young children and how many children are currently taking it.
DIET
If medications fail to control the seizures, then the next step is
often to try to control the seizures with diet. There is evidence that diet was used as
far back as ancient Greece to control seizures where the patients were told to fast and
eat just enough to stay alive. In 1911 a study was done in France that showed that dietary
changes to minimal calories could help epilepsy patients and after this more and more doctors
started recommending such measures. By 1921 serious research started being done to isolate
which dietary measures held the most promise - in particular they looked at the effects diet
had on diabetics.
When a person is starving and therefore has no carbohydrates available to burn for energy, the body
will begin to burn its stores of fats for energy. Similarly since diabetics cannot process sugar,
and sugar is a carbohydrate, they will also burn fat for energy. To some extent burning
fat isn't a problem and will just lead to weight loss, but if you take it to an extreme by
providing no carbohydrates then the body will start to produce things called ketones as a by-product
of burning the fat.
And it appears that once you get to the point where you are producing ketones, you are
also at a point where many people can achieve seizure control.
In high
concentrations ketones will actually change the pH of blood and if the pH becomes too low you
have a condition called ketoacidosis and that can lead to death so the trick is to produce
ketones at a high enough level to stop the seizures without going too far and causing illness.
This is why these diets should always be used under close supervision by your neurologist and
a dietician.
Like all seizure control methods there
are pros and cons. The diets actually have a fairly high success rate in controlling seizures
so that is a plus. The downside is that the diets are extraordinarily high in fat, have
some protein and very few carbs and the ratios of these items must be strictly followed.
If the child is tube fed it is relatively easy to maintain these ratios because they are
premeasured in the KetoCal formula. If they are not tube fed then their intake must be
strictly monitored and in most cases weighed very carefully.
I mention a few variations on the diet below, but they all require
large amounts of fat so the staples are things like whipping cream, butter, mayonnaise, eggs and other high
fat items with very little fruit or grains or other high carb items. For most people cheating
even a little bit can break ketosis and therefore seizure control will be lost. This diet
is also not really an option for people with dairy allergies unless they are tube fed
because all of the fat in the whipping cream, butter, eggs and mayo must be made up in oils.
Below is an overivew of the major diet options:
Ketogenic Diet
The Ketogenic Diet (keto) is usually described as a high fat, adequate protein,
low carbohydrate diet. And by high fat they mean a 4:1 ratio of fat to carbs/protein.
In other terms, the diet is usually around 90% fat.
Percentages vary depending on who you are quoting, but it seems that about 2/3 of
people have a significant reduction in the number of seizures that they experience,
and it has a good rate of stopping seizures altogether.
The diet is initiated in the hospital, with a 4 or 5 day admission during
which the ratios of fat to carbs and proteins are tweaked until they get the desired
number of ketones. The high fat diet is nutrient poor and so multivitamins must be
administered. Periodic blood tests must be administered to test for nutrient
levels and to check for ketoacidosis - a condition where the blood pH is lowered due to the
presence of too many ketones. To be certain that there is enough protein in the diet
for normal growth, weight and height must be monitored. Other possible side
effects are constipation, nausea and low energy due to lack of carbs.
MCT Diet
This diet is not usually used in the United States,
but is common in England and Canada. It works on the same principals as the ketogenic
diet, but it uses a different type of oil. The animal fats in the keto diet are
LCT's - Long Chain Triglycerides. The MCT diet is based on Medium Chain Triglycerides.
You don't need as many MCT's to produce the ketones as you do LCT's which is an
appealing aspect of the diet. However the MCT's come in the form of spreads and oils which
some find less appetizing and some say that the MCT's are harder on the tummy.
The MCT diet is a better solution for children with dairy allergies
because the oils are vegetable based. This diet is administered in much the same
way as the keto diet with the same precautions.
Modified Atkins Diet
This diet, also known as MAD was
developed by Dr. Eric Kossoff at Johns Hopkins. This doctor was very helpful to us,
answering questions via email even though he doesn't know us and Owen isn't his patient.
This diet also works on the basis of producing ketones, but is less restrictive on the
carbs than the classic keto. He found that many people were able to obtain relief
from their seizures while producing fewer ketones than on the keto diet.
It is still a high fat diet and still has very low carbs, just not quite as low as the
keto and the portion control is less strict than the keto and MCT diets.
Since it can produce the same side effects as the MCT and keto it must be monitored in the same way.
While many people do experience relief on this diet, it does have a bit lower of a success
rate than the classic keto and therefore some people will start on the MAD and then move to the
keto if they still need better control.
LGIT Diet
The Low Glycemic Index Treatment was developed in
2002 by Dr. Elizabeth Thiele and dietician Heidi Pfeifer at Massachusetts General Hospital in
Boston. This diet does not attempt to produce ketones, but still drastically reduces
the amount of carbs that a person eats. Since no one really understands why it is that
the keto diet works, no one is sure if ketones are the actual mechanism that stop the seizures.
There is a school of thought that says it isn't the ketones at all, but a lack of sugars
in the brain that stop the seizures. While the success rate isn't quite as high as the
classic keto, it does work well for many people. The ratios in this diet are 60-70% fat,
20-30% protein and 10% carbs. Portion size is used in a more general sense and weighing
is not required. Since ketones are not produced it is usually administered on an
outpatient basis, though you still have to watch for vitamin and mineral deficiency.
Many people take the path of trying the LGIT first, then moving to the MAD and finally
going to the keto if none of the previous two work. This way you are giving the least
restrictive the first try and then moving upward. Many others start at the classic keto
and then once they have seizure control start loosening up toward the MAD and LGIT
until they stop having control.
RESECTIVE SURGERY
An EEG can be used to diagnose the presence of seizure activity in the brain. It can
also be used to determine where the seizures begin in the brain. This is one of the
reasons that so many electrodes are used - so that they can try to pinpoint the exact
parts of the brain that are involved in a seizure. During a long term seizure study
the neurologist will attempt to watch a number of seizures to see if there is a single
"focal point" in the brain where all of the seizures begin. If you are lucky enough
to have your seizures all originating in one small area of the brain then a neurosurgeon
might be able to go in and remove that tiny portion of the brain - provided it isn't
somewhere important like a motor control center - so that it can no longer trigger seizures.
It is actually fairly rare that this will work for a child with extensive brain damage
due to hydrocephalus because the wiring problems tend to be widespread, but it is usually
worth the look at an EEG to see if it is an option.
DISCONNECTION SURGERY
Whereas resective surgery tries to remove the area of a brain that is triggering the
seizures, disconnection surgery attempts to remove the pathways that allow seizures to
move through the brain. The most common type of disconnection surgery is a corpus
callostomy. The corpus callosum
is the structure that separates the two hemispheres of the brain. Removing this
structure makes it considerably more difficult for seizures to pass from one side of the
brain to the other. Of course agensis (a failure to form) of the corpus callosum is
very common in kids with hydrocephalus so this isn't always an option either, but if
you have a corpus callosum then it can be removed.
VAGUS NERVE STIMULATOR
Also known as VNS, this is essentially a pacemaker for the brain. A small device is
implanted just below the collarbone on the left side with electrodes going up into the neck and
wrapping around the Vagus nerve.
Photo from Cyberonics, Inc.
An electrical pulse is sent out about every 5 minutes and lasts for around 30 seconds.
The interval, duration and strength of the pulses can be programmed using a magnetic wand
without the need for further surgery. These pulses reduce seizure activity in many people,
though no one knows why this works either. The wand can also be used to initiate a pulse at
the onset of a seizure, which will often stop the seizure or at least lessen its duration or severity
without the use of Diastat.
The procedure to place the implant is fairly low on the scale of surgeries that most hydrocephalus
patients are used to. It is done on an outpatient basis so that they are implanted and sent
home the same day without an admission to the hospital floor - although some neurosurgeons
will admit smaller children with shunts overnight just to be absolutely sure and may give
them some extra antibiotics just because where there is a shunt there is extra risk
of infection. Since they are working on the
chest and neck, the CSF is not touched and so there is minimal
(though of course there is always some) risk of a shunt infection.
The VNS does not have as high of a success rate as the diets in completely
stopping the seizures, but a large percentage do have at least some relief.
The device is not FDA approved for children, though it has been used in kids fairly
widely for many years, so there aren't any numbers to quote but our neurologist says
that it seems to work better in children than it does in adults in his experience.
The most common side effects are a change in the voice during the pulse, a tingling in the
neck during the pulse and coughs during the pulse. Since the amount of current being
applied is programmable they can work to set the levels to keep these effects to a minimum.
These side effects also seem to diminish in most people over time.
The VNS is usually (though not always) turned on at a very low current during the surgery. The
patient must then return about every two weeks to have the current slowly increased to therapeutic
levels. The amount of current required is different from one person to another so the
neurologist will come up with a plan specific to your child.
My Owen had a VNS placed just over a month ago at this writing. We have noticed a
marked increase in his ability to concentrate which means that the background activity has
most likely lessened. It has also had a good mood leveling effect - which is a known
byproduct of the VNS current. Finally while his seizures have not stopped - we are
not yet at therapeutic levels of current - their severity has decreased. His voice does
warble while it is pulsing but it doesn't seem to bother him, in fact he thinks it's funny.
It is possible to turn off the VNS at any time by placing the magnet over it. If you need
to turn it for an extended time, for example to keep your voice from warbling during a
concert or speech therapy, then you just tape the magnet over the VNS and it will stay off
as long as the magnet is there. As soon as you remove the magnet the VNS will restart on
its own.
Why Are Seizures With Hydrocephalus So Much Harder To Treat?
I get this question a lot. I'm not saying that anyone's seizures are a walk in the park, but
it is true that a higher percentage of kids with hydrocephalus have what they call
"intractable seizures" meaning that they do not respond well to medication. Is this true for
all kids with hydrocephalus, of course not, but we're certainly running higher than the
average population. I also often get asked why it is that seizures often don't show up until
the kids are two or three. This is how I picture the answer to both questions in my mind:
Picture a scenario in which you are asked to light up a large room.
You are handed a brand new spool of wire and 50 light bulbs.
You merrily go along connecting the wire to power and then hooking up each light
as you string them around the room. The room is beautifully lit when you are done
and the task is accomplished with relative ease. Now picture a situation where you are
asked to light up the same room, but are instead handed a big box full of a nest of old wire.
The insulation is cracked in places and the wires are all tangled up and you can't
straighten them out. You go about hooking up the first light, it's not too difficult to get a
wire that works all the way to the light. Now you hook up a second and a third.
Not too bad. By the time your get to the tenth light, it only comes on dimly and
the second light now seems to be dim too. The cracked insulation has allowed the
wires to cross and you have a power drain. Bummer, unhook the tenth light and try again.
By the time you hit the twentieth light things are dimming and shorts are causing lights
to pop. Each light becomes more and more difficult to get going without things going
haywire. You do finally get to 50 lights, but any sudden movement or disruption could
cause the whole thing to malfunction.
So you get the idea.
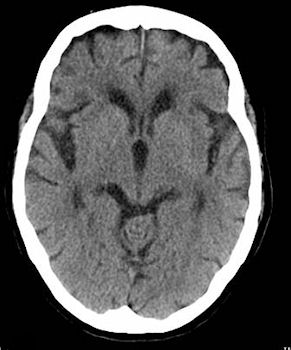
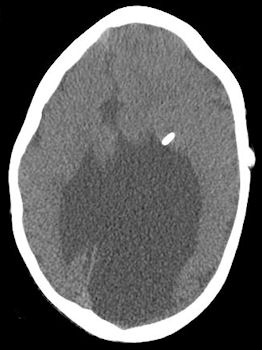
On the left is a CT of a normal brain, on the right is a CT of Owen's brain
(the shiny thing is his shunt).
The wiring in a brain that has been damaged by hydrocephalus is going to be a bit different.
When the children are very small and there are only so many neural pathways present, it is easier for the
brain to map those functions without causing any problems. As they get older and there are more pathways,
it can be harder for it to find ways around the damage. This is why our neurologist has warned us that
during times when Owen is learning things at a more rapid pace, we need to be more watchful of a seizure.
This is also one reason why so many people outgrow seizures as there isn't such a rapid creation of pathways when we get older.
The other reason that you don't see them in younger children was explained in my "How To Spot a Seizure"
section above - infants have very little muscle tone and therefore their symptoms tend to be more subtle
and can easily be missed.
Shunts and Seizures
There is one added concern for kids with shunts. A sudden appearance of seizures or
increase in seizure activity can be a sign of shunt failure. This is much like every
other sign of shunt failure - it might or might not mean there is a problem with the shunt.
Just as throwing up can be a sign of shunt failure or a sign that your precious little one
has brought home stomach bug, a sudden change in seizures could also mean that they have
outgrown their med dosage. So it's just one factor to take into account when thinking
about shunt failures.
What Should I Be Doing?
Other than the obvious step of getting your child to a neurologist for diagnosis and treatment, and
following that treatment to the letter there are a few other things you should be doing. The first
is to keep a log of all your child's seizures. If they are having quick ones that last only a few
seconds but are having 20 or more a day, then a daily log with general info about the overall
day is enough. If they are more rare but probably more spectacular you will want to write down the
time, the meds that they were on, the symptoms that they experienced (convulsions, which body
parts were convulsing, where did the convulsions start, how long did the convulsions last, did
the head or eyes turn to one side, did they vomit, did they have breathing problems, whatever
they experienced in a fair amount of detail). This kind of journal may seem like a hassle but
if there is one thing I have learned it is that memory is a fickle thing. It is very easy to think
"he never had seizures like this when he was on med x" because he just had a bad seizure and it
seemed awful. And then you go back over your log and realize that in fact he did have a seizure like that
on med x. It is also the only real way to spot patterns - do they have most of their seizures at
bedtimes, when they are sick or some other trigger. You can also see subtle changes in the severity
of the seizures on different meds so that you can see which ones worked best. This really is worth it.
Another thing you can do is to stay organized. If you need rescue meds, oxygen or
other support for seizures, always keep them in the same place - always. And get enough that
you can keep a set in each car and one at home so that you are never having to think - did I remember
to bring it? You will be busy one day and you will forget it. The exception is Diastat which is rather temperature sensitive. That shouldn't be
left in your car so you should upgrade that purse to something big enough to carry it with you.
You should also keep a list of current meds on you with their strengths and their dosages so that
in an emergency you don't have to remember it. I also keep copies of this list with me so that
I can just hand it to the docs without needing to write the darn thing out every time we pop in for a
visit.
Finally, and probably most importantly - take an Advanced CPR course - I highly recommend the
Red Cross Professional Rescuer Course. It's only $80 but it covers advanced recessitation.
You may never need it. Your
child may never have a seizure in their whole life. But if they do have one you don't have time
to be trained after the seizure starts. I actually recommend that every parent should at least
take the basic Red Cross CPR and First Aid course whether their child has a medical condition or
not just because we are sort of responsible for their well being and even healthy children have
accidents.
Legal Disclaimer: While every effort has been made to make certain that the information contained in this website is accurate, it must be remembered that the content is managed by a parent, not by a doctor. Information contained here is for general support purposes only and is no substitute for the care of a physician.